To date, the use of intravenous methylprednisolone has been the standard procedure for treating RR-MS. If it can alleviate the symptoms during episodes seen in multiple sclerosis patients, then it’s only logical to suggest that intermittent doses of intravenous methylprednisolone would decrease the severity of symptoms AND prevent future episodes in remitting relapsing MS. However, very little has been done so far to prove this theory about intermittent treatment with intravenous methylprednisolone, irrespective of an episode.
A recent study has tested it and proved it to be very effective in treating RR-MS. Further, it has demonstrated that intermittent methylprednisolone is the strategy to be relied upon to PREVENT future episodes. Given the remarkable changes following the strategy tested, it is safe to say that patients whose disease seems to follow the clinical course of RR-MS can now look forward to having fewer and milder episodes in future. In addition to decreasing the number of lesions (by 14% to 100 %), there is also a marked decrease in prolactin levels. Decreased prolactin levels prevent auto-immunity that is characteristic of the episodes in RR-MS patients.
Background
Four different types of Multiple Sclerosis have been described, based on the clinical progression of the disease. One of them is Relapsing-remitting.
The study in question focused on relapsing-remitting or RR-MS. It happens to be the most common kind, seen in 85% of the cases. It is characterized by episodes of relapses. With each relapse, the patient stands to be disabled temporarily and in some severe cases, permanently. At the histological level, RR-MS patients show lesions in the brain, a high T2 volume load and finally high levels of prolactin. High levels of the hormone in plasma cause surges in the levels of auto-immunity.
As early as 1987, methylprednisolone was administered intravenously to combat the symptoms in all four kinds of MS. The strategy thus far was to use intravenous methylprednisolone following an episode with tapering oral doses for three to five days. This standard treatment with following an episode also decreases the levels of prolactin in the plasma. While intermittent intravenous methylprednisolone seemed to be the obvious choice to prevent future episodes, no study was under-taken to actually test such a strategy.
Nine patients were recruited for this open, single crossover study that lasted for one year.
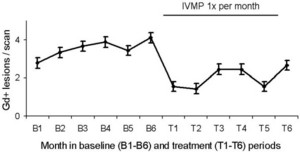
They underwent cranial Gd-MRIs every month for twelve months. Half-way through, after six months, the patients were given 500 mg of I.V. methylprednisolone, followed by an oral tapering dose for 3 days after the MRI.
The focus of the study was to look for differences in Gd-enhancing lesions, T2 lesion volume and finally prolactin levels. The mean number of Gd+ lesions before treatment was measured against the number prior to treatment. The same was true for T2 lesion volume.
Study Design
This study was designed to see if the intermittent administration of intravenous methylprednisolone would decrease the number of Gd-enhancing lesions in RR-MS patients. This was based on an isolated study carried out in 1987 on optic neuritis. Following the positive effects of intravenous methylprednisolone in a three to five day course, it was obvious that an intermittent administration of methylprednisolone might keep the number of lesions to a minimum. This was the primary focus of the study.
In addition to Gd-enhancing lesions, patients suffering from RR-MS also display high levels of prolactin in their plasma. This leads to auto-immunity. Hence only those patients who had not been given immune-suppressants were selected to participate in the study.
Comparison group
The group that underwent treatment was compared with patients from the Sylvia Lawry MS database. Patients who had a Gd+ enhancing lesion in the first month and developed one or more lesion in the following three months were selected. These selection criteria yielded a total of eighty-three patients. What makes the results of this study so ideal for application in near future is that the comparison group was treated with intravenous methylprednisolone only after a relapse, but these patients did not show a decrease either in
1) The number of Gd-enhancing lesions or
2) T2 lesion volume
In addition to these, the plasma levels of the hormone prolactin were also measured.
Thus, the administration of intravenous methylprednisolone (500mg) following an episode only alleviated the acute symptoms. The intermittent intravenous methylprednisolone strategy decreased the number of lesions.
One of the major doubts surrounding such a strategy is whether such prolonged use of corticosteroids will be well tolerated by the patients (the strategy described here is a MONTHLY ADMISISTRATION OF intravenous methylprednisolone, regardless of an episode).
For six months,initially, the patients were merely subjected to cranial Gd-MRI, formed the BASELINE study. for the next few months, months six through eleven, the TREATMENT part of the study was carried out. They were under observation for the number of lesions and T2 lesion load. Further, these patients were also compared to eighty three patients from the Sylvia Lawry MS database.
Surprisingly, these comparisons revealed that not only was it well-tolerated but the stringent safety tests also indicated that a monthly administration of methylprednisolone does not put the patient at a risk. The mean number of lesions was decreased by 46% and the median number of lesions was decreased by 43%.
Data
Since the patients were being tested for the effect of the treatment, a signed paired non-parametric Wilcoxon test was used to measure the differences. p= 0.05 was accepted. Prior to analysis of variance the continuous variables were transformed.
Lesion Load
What sets this study a cut above the rest is that this is the first study to show that T2 lesion load can be decreased via a monthly administration of intravenousmethylprednisolone. A high dose of glucocorticoids has a terrible side effect. It causes dehydration, thus bringing about pseudo-atrophy. Previous short and long term treatments did not have this positive effect on lesion load. In addition, reports in 1989 and 2002 showed that anti-edematous effect was observed during treatment with intravenousmethylprednisolone during acute exacerbations. Thus, edema resolution can be ruled out as one of the factors contributing to the change in T2 signal.
Prolactin Levels
A study published in 1999 showed that MS patients displayed high levels of the hormone prolactin during relapses. (Azar ST, Yamout B. Prolactin secretion is increased in patients with multiple sclerosis. Endocr Res. 1999;25:207-14. [PubMed])
This monthly intermittent treatment caused patients to show a remarkable decrease in the serum levels of the hormone prolactin.
RR-MS patients are seriously affected by the symptoms seen during an episode. The lesions in their brain are only temporarily decreased under the traditional treatment method of using intravenousmethylprednisolone following an episode. Up until now there has been no way of preventing future episodes which are very debilitating while they last. This recent study by Florian Then Bergh et al showed that monthly administrations of intravenousmethylprednisolone irrespective of an episode in RR-MS patients can PREVENT FUTURE EPISODES.
This is the only study that has shown that a monthly administration of intravenousmethylprednisolone can decrease T2 lesion load.
This study further proved that patients with active lesions and high prolactin levels during episodes showed a reversal of the symptoms after undergoing the monthly treatment regimen for six months. This raises some serious questions such as: Will the long term usage of methylprednisolone have deleterious side effects? Should RR-MS patient undergo this regimen for life?
While the later question has not been answered in this study, the former was addressed very clearly. This study also carried out safety studies and showed this treatment to be devoid of negative side effects generally associated with the long term use of methylprednisolone. Given these results, the day is not far when this strategy will be adopted to treat and prevent future episodes in RR-MS patients, thus decreasing episodes of disruptions. MS patients can look forward to more normal life, should this strategy meet with approval.
Reference:
www.pubmed.govwww.ncbi.nlm.nih.gov BMC Neurol. 2006 May 23;6:19 Monthly i.v. methylprednisolone in relapsing-remitting MS – Reduction of enhancing lesions, T2 lesion volume and plasma prolactin concentrations. Florian Then Bergh, Tania Kuempfel, Erina Schumann, Ulrike Held, Michaela Schwan, Mirjana Blazevic, Axel Wismueller, Florian Holsboer, Alexander Yassouridis, Manfred Uhr, Frank Weber, Martin Daumer, Claudia Trenkwalder, Dorothee Auer