When my daughter and son-in-law went for their nineteen-week routine prenatal ultrasound, they were excited to find out the sex of their baby. They were told the baby is a girl, and also that she has a birth defect called Congenital Diaphragmatic Hernia, or CDH. Since that time we have read and researched every possible source we could find for CDH. We have talked to obstetricians, pediatricians, pediatric surgeons, and other CDH mothers. What we have learned is that much of the information available on the internet is outdated or inaccurate. I can tell you what we have learned.
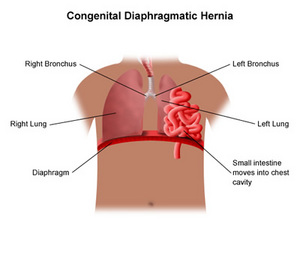
Congenital Diaphragmatic Hernia occurs in 1 out of every 2500 births. It occurs in every race, religious background, and economic level. It also does not correspond to the prenatal care the mother receives. No one knows what causes it, although there are major research studies being done to try to find the cause. In approximately the tenth week of fetal development, the diaphragm forms. The diaphragm is a muscle that separates the heart and lungs in the chest cavity from the organs in the abdominal cavity. With CDH babies, there is a hole in the diaphragm, and this opening allows some of the organs such as the stomach, liver, or intestines to move up into the chest cavity and take up space where the lungs should be developing. Most hernias are left-sided, but a small percentage is right-sided. They can vary from a mild defect to severe, but most doctors agree that there are no real statistics as to how well any certain baby will do until the baby is born and determination is made about how well that baby’s lungs function.
Some websites we researched set the mortality rate at 50%, some say 75% survive, others say 85% and still others 93%. So much depends on how much of the organs have moved into the chest cavity, how well the lungs that develop can mature, and whether that baby has other chromosomal issues. Usually the expectant mother will have an amniocentesis to determine if there are other abnormalities. Some of these babies have other problems related to the CDH, such as feeding problems, or short term or long term oxygen dependency. Some severe cases are ventilator dependent. Some babies have no complications other than the small scar to repair the hernia.
Usually the baby is born and taken immediately to the NICU, where the baby is stabilized. Some babies need ventilation. Some babies require ECMO, or Extracorpreal Membrane Oxygenation, which is available in some larger medical centers. ECMO is a heart/lung bypass machine, that can add oxygen to the baby’s blood and remove carbon dioxide, much as heart patients receive when having open heart surgery. When it becomes necessary to put a baby on ECMO, his or her lungs have a chance to rest and continue to mature. A pediatric surgeon told us that babies lungs can continue to develop and mature until the child is around eight years of age. ECMO is usually a short-term treatment because of the blood-thinning medicines required, but it can be life saving.
In the best case scenario, Congenital Diaphragmatic Hernia is diagnosed in utero, and the baby is born to a waiting pediatric team prepared to care for the CDH baby. The mother is usually giving the genetic testing and delivers as a high-risk pregnancy. In some cases, however, the condition is not diagnosed until after birth. In these cases, the babies are usually transferred to a high-risk neonatal intensive care unit at the nearest large medical center.
My daughter will be delivering at a large medical center. The pediatricians we spoke with took us on a tour of the NICU and gave us some idea of how the defect can vary from mild to severe. One baby we saw there had been a “worst case” and another had been a “best case” of the fifteen or so CDH babies they had treated in the last four months. Out of the fifteen, two of the babies did not survive. Both had severe cases of CDH. The baby they considered a “best case” was stabilized and had the corrective surgery on the sixth day. At ten days of age, the baby was discharged with only small scars from the surgery.
Surgery to repair the hernia must be done, but doctors do not rush to do this. They now feel that the babies need to have a chance to stabilize and adjust to life outside the womb and the treatments before they have surgery. Many babies wait for weeks to have the surgery. We were told the average hospital stay for most CDH babies at that hospital was two months.
Mothers who deliver a CDH baby statistically have a 2% chance of delivering another CDH baby, although doctors have not determined a genetic cause.
Mothers who have delivered babies with CDH have banded together to support each other on a couple of websites. Cherubs has a wealth of information and is updated frequently. There is also a support group online called Breath of Hope. Other mothers are so helpful in sharing their experiences.
My daughter has not delivered yet, so we are just waiting. This is an anxious time for all of our family. I can tell you that if your baby was diagnosed with this condition, don’t let the dire statistics on some websites discourage you. Find out all you can about the severity of your baby’s particular defect. Make arrangements to deliver at a hospital with the facilities to treat CDH babies. Find other mothers to support you. Cry when you need to, but don’t give up hope.
A hospital has an excellent video available to watch online about CDH. It is located here. Your CDH baby is special and may have special challenges, but you are not alone.






