Diagnosed with Common Variable Immune Deficiency (CVID) in 1994, I soon became a patient advocate for this frequently misunderstood and undiagnosed illness. Oddly enough, the organization I first worked with was U.K. based, and I happen to be a U.S. resident.
Call me selfish, but at the ripe old age of 25 I was not quite yet ready to throw in the towel. Medical knowledge concerning CVID has improved considerably – thanks to patient organizations such as the Immune Deficiency Foundation.
Yet patients continue to experience delayed diagnosis and treatment as well as insurance coverage difficulties.
Contents:
–Overview of Immune Deficiency
–CVID Symptoms
–CVID Diagnosis
–Difficulties in Diagnosis
–CVID Treatment
–Treatment Complications
–Living with CVID
–Child-Friendly Help
Hypogammaglobulinemia – Overview
Hypogammaglobulinemia essentially means antibody deficiency, and includes numerous primary immune deficiency diseases such as Common Variable Immune Deficiency (CVID). Unlike AIDS or chemotherapy-induced immune deficiency, primary immune deficiencies are considered inherent, perhaps genetic.
One of the rarest forms of hypogammaglobulinemia, Severe Combined Immune Deficiency, is nicknamed the “boy-in-the-bubble” disease – a somewhat popular example known to movie viewers.
Both Common Variable Immune Deficiency (CVID) and IgA deficiency, whereas antibodies are decreased but not absent, are much more common. The approximate rate for CVID is 1:50,000 persons and the rate for IgA deficiency is as frequent as 1:750 individuals.
As the immune system is quite complex, CVID often involves additional defects in the immune system.
Common Variable Immune Deficiency (CVID) is mild to life-threatening: dependent on resistance to infection, treatment success, and if complications occur. Significant risk of developing certain cancers and autoimmune illness also exists for patients.
Children with CVID are typically born with the immune deficiency but adult-onset CVID is not uncommon. The exact cause of CVID is unknown but genetic factors are implicated.
Understanding Immune Globulins and Antibodies in CVID
(Refer to the end of the article for a child-friendly explanation)
The immune system consists of five primary types of antibodies called immune globulins, two of which are commonly affected in CVID: immune globulin G (IgG) and immune globulin A (IgA). IgM deficiency occurs less frequently, though up to 50 percent of the time.
Each antibody class plays a different role in response to infection:
— IgA is the chief protector of mucosal linings, including the mouth, stomach, respiratory tract, intestines, and external reproductive organs.
— IgG is the body’s main defense antibody throughout the body. Some CVID patients mount little to no antibody response to both common and dangerous bacteria — causing pneumonia, tetanus, strep, and colds, for instance.
Symptoms of Common Variable Immune Deficiency
— frequent and chronic bacterial, viral or fungal infections (bronchitis, pneumonia, conjunctivitis, colds, influenza, ear infections, skin infections etc.)
Symptoms for mild to moderate CVID and IgA deficiency may be similar. However, there is no treatment for IgA deficiency other than keeping an upper-hand on infections with antibiotic therapy.
Diagnosis of Common Variable Immune Deficiency
Testing is done by measuring immune globulin levels in the blood. Supportive tests such as antibody response tests and CT scan of sinus or lungs may also be utilized.
Whether testing is underutilized or the total immunoglobulin level is misinterpreted, both contribute to diagnosistic delay.
Additionally, the total IgG or IgA count can be misleading, and these levels alone are not necessarily indicative of the patient’s health status.
As each immune globulin class is divided into subclasses, sometimes one subclass is abundantly produced while one or more other subclasses remain deficient or absent. A more refined test, called an IgG subclass level, is often necessary to pinpoint CVID.
Additionally, treatment of CVID is very costly (thousands of dollars monthly). Insurance companies may refuse treatment if antibody levels are not considered “low enough,” and physicians can be misled as to what constitutes CVID.
Treatment for Common Variable Immune Deficiency
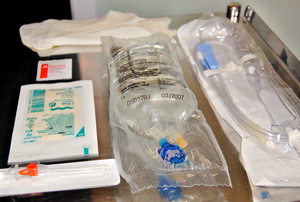
Some antibodies may be replaced by what is known as intravenous immune globulin (IVIG). IVIG is a very refined blood product gathered from a select pool of donors. Other forms of administration, such as subcutaneous injection under the skin, is less frequently involved.
Whereas IgG antibodies can be replaced, no replacement for IgA is available.
IVIG is optimally administered on a bi-weekly to monthly basis. Infusions typically last a few hours and temporary side effects, such as flu-like symptoms, are common.
Immune therapy replacement is not a cure for CVID; Generally, IVIG therapy is a lifelong treatment that helps patients’ better ward off infections and complications of the disease.
Most patients are healthier on IVIG, and some lead rather normal lives other than the inconvenience attributed to the infusions.
The majority of CVID patients ultimately experiences some degree of disability, from mild to severe, and maintain higher than normal rates of infection.
The earlier CVID patients receive IVIG the better the prognosis. With adequate treatment, sinus and lung damage as well as other complications may be prevented.
Prompt administration of antibiotics when necessary and regular evaluation by an immunologist or specialist is another crucial form of treatment for CVID patients.
Treatment Complications
Slower administration of IVIG and preemptive administration of diphenhydramine HCL (Benedryl) can greatly minimize infusion-related reactions. Ibuprofen or asprin may also be recommended.
More serious or life-threatening IVIG reactions occur in a smaller number of patients. The latter group may be unable to receive immune globulin therapy due to natural antibodies that react to trace amounts of IgA or other substances contained in immune globulin products.
Children and CVID
Kids with CVID have different educational, medical and support needs than do adult CVID patients. Just the difficulties involved with germ exposure during play or school are considerable. Additionally, peer pressure can make a child feel inadequate. For additional help consider support groups with dedicated information for parents and children. Parents may find both the Jeffrey Modell Foundation and the IDF quite helpful.
For a fantastic, child-oriented explanation of the immune system see “Our Immune System,” by the Immune Deficiency Foundation (IDF). Incidentally, many adults like it too.
 - when Germs Are a Threat")



